Background: The malaria diagnostic tools developed to date require blood to be taken. However, certain groups in the population are reluctant to take blood samples because of their cultural habits (blood taboo), or because of the fear associated with the trauma of the injection, especially when the sample is taken repeatedly. Saliva and urine, which are not very invasive to collect, have not been widely used for malaria diagnosis. The aim of this study is to assess the performance of saliva and urine in detecting molecular markers of Plasmodium falciparum resistance to antimalarial drugs. Methodology: Blood, urine and saliva samples were collected in three different localities from 94 patients over 2 years of age with microscopically confirmed Plasmodium falciparum uncomplicated malaria. P. falciparum genomic DNA (Deoxyribonucleic acid) was then extracted and amplified using primers specific for the Pfcrt (Plasmodium falciparum Chloroquine Resistance Transporter), Pfdhfr (Plasmodium falciparum dihydrofolate reductase) and PfK13 propeller (Plasmodium falciparum Kelch13 propeller) genes. The amplification products were processed by electrophoresis and analyzed against blood, saliva and urine samples. A multivariate statistical analysis in R programming environment was performed aiming to assess the performance of blood, saliva and urine samples in detecting molecular markers of P. falciparum resistance. Results: Agarose gel electrophoresis of the amplification products of each gene detected the Pfcrt genes at 80.85% (76/94), Pfdhfr at 95.74% (90/94) and PfK13 Propeller at 98.93% (93/94) in blood. In saliva, gene detection levels were 50% (47/94), 69.14% (65/94) and 4.26% (4/94) respectively for the K13 propeller, Pfdhfr and Pfcrt genes. Unlike the Pfcrt gene, which was not detected, 45.74% (43/94) and 38.30% (36/94) of PfK13 Propeller and pfdhfr genes respectively were detected in urine. Taking blood as the reference biological sample, statistical analysis showed that unlike urine, saliva exhibited a detection performance for molecular markers of antimalarial drug resistance (pfcrt, pfdhfr, pfK13 propeller) close to that of blood (p < 0.05). The performance of saliva and urine was also assessed on the basis of the detection of the molecular markers pfdhfr, pfcrt and pfK13 using ROC (receiver operational characteristic) analysis. The data revealed a high sensitivity of saliva compared with urine in the detection of the pfdhfr, pfcrt and pfK13 propeller genes. Conclusion: The levels of detection of molecular markers of antimalarial drug resistance studied in saliva are close to those in blood. Saliva is a high-performance biological product that could potentially be used as an alternative non-invasive sample for the study of molecular markers of Plasmodium falciparum resistance to antimalarial drugs.
| Published in | International Journal of Microbiology and Biotechnology (Volume 9, Issue 3) |
| DOI | 10.11648/j.ijmb.20240903.14 |
| Page(s) | 68-78 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Saliva, Urine, Malaria, Diagnosis, Plasmodium falciparum, Pfcrt, Pfdhfr and PfK13
Sites | Collection period | Age groups | Average age (years) | Number of patients | Types of samples | Number of samples collected |
|---|---|---|---|---|---|---|
Blood | 52 | |||||
Anonkoua-kouté | February – March 2015 | 2 to 53 years | 16,60 | 52 | Saliva | 52 |
Urine | 52 | |||||
Blood | 51 | |||||
Port - Bouët | April - May – June 2015 | 2 to 62 years | 16,69 | 51 | Saliva | 51 |
Urine | 51 | |||||
Blood | 50 | |||||
Ayamé | June - July – August 2015 | 2 to 55 years | 15,84 | 50 | Saliva | 50 |
Urine | 50 | |||||
Total | 153 | 459 |
k13sg | k13sl | dhfrsg | dhfrsl | crtsg | DP | k13ur | dhfrur | |
|---|---|---|---|---|---|---|---|---|
k13sg | 1 | |||||||
k13sl | 0,10 | 1 | ||||||
dhfrsg | 0,40* | -0,01 | 1 | |||||
dhfrsl | -0,07 | 0,05 | 0,20* | 1 | ||||
crtsg | 0,20* | 0,30* | 0,14 | 0,12 | 1 | |||
DP | 0,05 | 0,17* | 0,11 | 0,06 | 0,21* | 1 | ||
k13ur | 0,10 | -0,04 | 0,07 | 0,01 | 0,12 | -0,11 | 1 | |
dhfrur | 0,08 | -0,01 | 0,11 | -0,10 | 0,02 | -0,07 | -0,0004 | 1 |
Parameters | Saliva | Urine | ||||
|---|---|---|---|---|---|---|
Pfk13 | pfdhfr | pfcrt | Pfk13 | pfdhfr | Pfcrt | |
Sensitivity | 0,46 | 0,64 | 0,05 | 0,45 | 0,38 | 0 |
Specificity | 0,2 | 0,5 | 0,5 | 0,5 | 0,5 | 0,01 |
Accuracy | 0,43 | 0,54 | 0,05 | 0,45 | 0,38 | 0,01 |
Positive Predictive Value (PPV) | 0,91 | 0,98 | 0,8 | 0,95 | 0,94 | 0 |
Pfcrt | Plasmodium Falciparum Chloroquine Resistance Transporter |
Pfdhfr | Plasmodium Falciparum Dihydrofolate Reductase |
Pfk13 propeller | Plasmodium Falciparum Kelch13 Propeller |
PCR | Polymerase Chain Reaction |
DNA | Deoxyribonucleic Acid |
ELISA | Enzyme-Linked Immuno-Sorbent Assay |
EDTA | Ethylene Diamine Tetra-Acetic Acid |
| [1] |
WHO. World Malaria Report 2023: Information pack, regional data and trends. [online]. Available:
https://cdn.who.int/media/docs/default-source/malaria/world-malaria-reports/world-malaria-report-2023-regional-briefing-kit-fre.pdf?sfvrsn=299150e7_15&download=true [Accessed November 2023] |
| [2] |
WHO, T3: test. treat. track. Scaling up diagnostic testing, treatment and surveillance for malaria. [online]. Available:
https://www.who.int/malaria/publications/atoz/t3_brochure/en/ [Accessed 23 Dec 2020] |
| [3] | Graz B, Willcox M, Szeless T, et al.. 'Test and treat' or presumptive treatment for malaria in high transmission situations? A reflection on the latest WHO guidelines. Malaria Journal, 2011; 10: 136. |
| [4] | Putaporntip C., Buppan P., Jongwutiwes S., Improved performance with saliva and urine as alternative DNA sources for malaria diagnosis by mitochondrial DNA-based PCR assays. Clinical Microbiology and Infection, 2011, 17: 1484-1491. |
| [5] | Boahen O, Owusu-Agyei S, Febir LG, et al. Community perception and beliefs about blood draw for clinical research in Ghana. Transactions of the Royal Society of Tropical Medicine and Hygiene, 2013; 107: 261-5. |
| [6] | Chatio S, Baiden F, Achana FS, et al. Knowledge and perceptions about clinical trials and the use of biomedical samples: findings from a qualitative study in rural Northern Ghana. PLoS One, 2016; 11: e0152854. |
| [7] | Baiden F, Owusu-Agyei S, Okyere E, et al. Acceptability of rapid diagnostic test-based management of malaria among caregivers of Under-Five children in rural Ghana. PLoS One, 2012; 7: e45556. |
| [8] | Newton S, Doku V, Geissler W, et al. Drawing blood from young children: lessons learned from a trial in Ghana. Transactions of the Royal Society of Tropical Medicine and Hygiene, 2009; 103: 497-9. |
| [9] | Achieng F, Rosen JG, Cherop RY, et al. Caregiver and community perceptions and experiences participating in an infant malaria prevention trial of PfSPZ vaccine administered by direct venous inoculation: a qualitative study in Siaya County, Western Kenya. Malaria Journal, 2020; 19: 226. |
| [10] | Mharakurwa S., Simoloka C., Thuma P. E., Shiff C. J., Sullivan D. J., PCR detection of Plasmodium falciparum in human urine and saliva samples. Malaria Journal, 2006, 5: 103. |
| [11] | Nwakanma D. C., Gomez-Escobar N., Walther M., Crozier S., Dubovsky F., Malkin E., Locke E., Conway D. J., Quantitative detection of Plasmodium falciparum DNA in saliva, blood, and urine. Journal of Infectious Diseases, 2009, 199(11): 1567-74. |
| [12] | Aninagyei E, Abraham J, Atiiga P, et al. Evaluating the potential of using urine and saliva specimens for malaria diagnosis in suspected patients in Ghana. Malaria Journal, 2020; 19: 349. |
| [13] | Al-Shehri H, Power BJ, Archer J, et al. Non-invasive surveillance of Plasmodium infection by real- time PCR analysis of ethanol preserved faeces from Ugandan school children with intestinal schistosomiasis. Malaria Journal, 2019; 18: 109. |
| [14] | Adja A. M., N'goran E. K., Koudou B. G., Dia I., Kengne P., Fontenille D., Chandre F., Contribution of Anopheles funestus, An. gambiae and An. nili (Diptera: Culicidae) to the perennial malaria transmission in the southern and western forest areas of Côte d'Ivoire. 2011, Annals of Tropical Medicine and Parasitology, 105: 13-24. |
| [15] | Miguel R. H.; Coura J. R., Samudio F., Suárez-mutis M. C., Evaluation of three different DNA extraction methods from blood samples collected in dried filter paper in Plasmodium subpatent infections from the Amazon region in Brazil. Revista do Instituto de Medicina Tropical de São Paulo, 2013, 55(3): 205-8. |
| [16] | Kain K. C. & Lanar D. E., Determination of genetic variation within Plasmodium falciparum by using enzymatically amplified DNA from filter paper disks impregnated with whole blood. Journal of Clinical Microbiology, 1991, 29: 1171-1174. |
| [17] | Plowe C. V. & Wellems T. E., Molecular approaches to the spreading problem of drug resistant malaria. Advances in Experimental Medicine and Biology, 1995, 390: 197-209. |
| [18] | R Core Team, A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. ISBN 3-900051-07-0, URL accessed on 18 February 2017 at |
| [19] | Noel D. D., Inza J. F., Nafan D., Mohamed L. B., Jean-Luc A. M., Olefongo D., Loukou N. E., Martial D. S. Y., Souleymane S., Giovanni M., A Quick Computational Statistical Pipeline Developed in R Programing Environment for Agronomic Metric Data Analysis. American Journal of Bioinformatics Research 2019, 9(1): 22-44 |
| [20] | Dago Dougba Noel, Lallié Hermann Désiré N. M., Diarrassouba Nafan, Silué Souleymane and Giovanni Malerba. Correlation between accuracy sensitivity specificity and positive predictive value parameters in detecting differentially expressed genes. International Journal of Development Research, 2015, Vol. 5, Issue, 03, pp. 3734-3739, March, 2015. Available online at |
| [21] | Zahra G. N., Hormozd O., Lame A., Ahmad R. M., Ahmad R., Zahra R., Mehdi N., Elham R., Mitochondrial PCR-based malaria detection in saliva and urine of symptomatic patients. Transactions of the Royal Society of Tropical Medicine and Hygiene, 2014, 108: 358-362. |
| [22] |
Kwannan Nantavisai, Malaria detection using non-blood samples. Songklanakarin. Journal of Science and Technology, 2014, 634 36 (6): 633-641.
https://www.thaiscience.info/journals/Article/SONG/10968355.pdf |
| [23] | A-Elgayoum, S. M., El-Rayah, E.-A., Giha, H. A., Towards a noninvasive approach to malaria diagnosis: detection of parasite DNA in body secretions and surface mucosa. Journal of Molecular Microbiology and Biotechnology, 2010, 18, 148-155. |
| [24] | Sutherland C. J., Hallett, R., Detecting malaria parasites outside the blood. Journal of Infectious Diseases, 2009, 199, 1561-3. |
| [25] | Nguansangiam S., Day N. P., Hien T. T., Mai N. T., Chaisri U., Riganti M., Dondorp A. M., Lee S. J., Phu N. H., Turner G. D., White N. J., Ferguson D. J., Pongponratn E., A quantitative ultrastructural study of renal pathology in fatal Plasmodium falciparum malaria. Tropical Medicine and International Health, 2007, 12, 1037-50. |
| [26] | Das B. S., Renal failure in malaria. Journal of Vector Borne Diseases. 2008, 45, 83-97. |
| [27] | Kawai Satoru, Megumi Sato, Naoko Kato-Hayashi, Hisashi Kishi, Michael A. Huffman, Yoshimasa Maeno, Richard Culleton, Shusuke Nakazawa, Detection of Plasmodium knowlesi DNA in the urine and faeces of a Japanese macaque (Macaca fuscata) over the course of an experimentally induced infection. Malaria Journal, 2014, 13: 373. |
| [28] | Danwang C, Noubiap JJ, Souopgui J, et al. Accuracy of malaria diagnostic tests performed on noninvasively collected samples: a systematic review and metaanalysis. BMJ Global Health, 2021; 6: e005634. |
| [29] | Bousema T., Okell L., Felger I., Drakeley C., Asymptomatic malaria infections: detectability, transmissibility and public health relevance. Nature Reviews Microbiology, 2014, 12(12): 833-840. |
APA Style
Oléfongo, D., Noél, D. D., Angélo, K. K. B., Bérenger, A. A. A. A., Kouakou, B., et al. (2024). Assessment of Saliva and Urine Performance for Antimalarial Drug Resistance Molecular Markers Study. International Journal of Microbiology and Biotechnology, 9(3), 68-78. https://doi.org/10.11648/j.ijmb.20240903.14
ACS Style
Oléfongo, D.; Noél, D. D.; Angélo, K. K. B.; Bérenger, A. A. A. A.; Kouakou, B., et al. Assessment of Saliva and Urine Performance for Antimalarial Drug Resistance Molecular Markers Study. Int. J. Microbiol. Biotechnol. 2024, 9(3), 68-78. doi: 10.11648/j.ijmb.20240903.14
AMA Style
Oléfongo D, Noél DD, Angélo KKB, Bérenger AAAA, Kouakou B, et al. Assessment of Saliva and Urine Performance for Antimalarial Drug Resistance Molecular Markers Study. Int J Microbiol Biotechnol. 2024;9(3):68-78. doi: 10.11648/j.ijmb.20240903.14
@article{10.11648/j.ijmb.20240903.14,
author = {Dagnogo Oléfongo and Dago Dougba Noél and Kouman Kouamé Bouatini Angélo and Ako Ako Ako Aristide Bérenger and Bla Kouakou and Touré Offianan André and Djaman Allico Joseph},
title = {Assessment of Saliva and Urine Performance for Antimalarial Drug Resistance Molecular Markers Study
},
journal = {International Journal of Microbiology and Biotechnology},
volume = {9},
number = {3},
pages = {68-78},
doi = {10.11648/j.ijmb.20240903.14},
url = {https://doi.org/10.11648/j.ijmb.20240903.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmb.20240903.14},
abstract = {Background: The malaria diagnostic tools developed to date require blood to be taken. However, certain groups in the population are reluctant to take blood samples because of their cultural habits (blood taboo), or because of the fear associated with the trauma of the injection, especially when the sample is taken repeatedly. Saliva and urine, which are not very invasive to collect, have not been widely used for malaria diagnosis. The aim of this study is to assess the performance of saliva and urine in detecting molecular markers of Plasmodium falciparum resistance to antimalarial drugs. Methodology: Blood, urine and saliva samples were collected in three different localities from 94 patients over 2 years of age with microscopically confirmed Plasmodium falciparum uncomplicated malaria. P. falciparum genomic DNA (Deoxyribonucleic acid) was then extracted and amplified using primers specific for the Pfcrt (Plasmodium falciparum Chloroquine Resistance Transporter), Pfdhfr (Plasmodium falciparum dihydrofolate reductase) and PfK13 propeller (Plasmodium falciparum Kelch13 propeller) genes. The amplification products were processed by electrophoresis and analyzed against blood, saliva and urine samples. A multivariate statistical analysis in R programming environment was performed aiming to assess the performance of blood, saliva and urine samples in detecting molecular markers of P. falciparum resistance. Results: Agarose gel electrophoresis of the amplification products of each gene detected the Pfcrt genes at 80.85% (76/94), Pfdhfr at 95.74% (90/94) and PfK13 Propeller at 98.93% (93/94) in blood. In saliva, gene detection levels were 50% (47/94), 69.14% (65/94) and 4.26% (4/94) respectively for the K13 propeller, Pfdhfr and Pfcrt genes. Unlike the Pfcrt gene, which was not detected, 45.74% (43/94) and 38.30% (36/94) of PfK13 Propeller and pfdhfr genes respectively were detected in urine. Taking blood as the reference biological sample, statistical analysis showed that unlike urine, saliva exhibited a detection performance for molecular markers of antimalarial drug resistance (pfcrt, pfdhfr, pfK13 propeller) close to that of blood (p pfdhfr, pfcrt and pfK13 using ROC (receiver operational characteristic) analysis. The data revealed a high sensitivity of saliva compared with urine in the detection of the pfdhfr, pfcrt and pfK13 propeller genes. Conclusion: The levels of detection of molecular markers of antimalarial drug resistance studied in saliva are close to those in blood. Saliva is a high-performance biological product that could potentially be used as an alternative non-invasive sample for the study of molecular markers of Plasmodium falciparum resistance to antimalarial drugs.
},
year = {2024}
}
TY - JOUR T1 - Assessment of Saliva and Urine Performance for Antimalarial Drug Resistance Molecular Markers Study AU - Dagnogo Oléfongo AU - Dago Dougba Noél AU - Kouman Kouamé Bouatini Angélo AU - Ako Ako Ako Aristide Bérenger AU - Bla Kouakou AU - Touré Offianan André AU - Djaman Allico Joseph Y1 - 2024/08/20 PY - 2024 N1 - https://doi.org/10.11648/j.ijmb.20240903.14 DO - 10.11648/j.ijmb.20240903.14 T2 - International Journal of Microbiology and Biotechnology JF - International Journal of Microbiology and Biotechnology JO - International Journal of Microbiology and Biotechnology SP - 68 EP - 78 PB - Science Publishing Group SN - 2578-9686 UR - https://doi.org/10.11648/j.ijmb.20240903.14 AB - Background: The malaria diagnostic tools developed to date require blood to be taken. However, certain groups in the population are reluctant to take blood samples because of their cultural habits (blood taboo), or because of the fear associated with the trauma of the injection, especially when the sample is taken repeatedly. Saliva and urine, which are not very invasive to collect, have not been widely used for malaria diagnosis. The aim of this study is to assess the performance of saliva and urine in detecting molecular markers of Plasmodium falciparum resistance to antimalarial drugs. Methodology: Blood, urine and saliva samples were collected in three different localities from 94 patients over 2 years of age with microscopically confirmed Plasmodium falciparum uncomplicated malaria. P. falciparum genomic DNA (Deoxyribonucleic acid) was then extracted and amplified using primers specific for the Pfcrt (Plasmodium falciparum Chloroquine Resistance Transporter), Pfdhfr (Plasmodium falciparum dihydrofolate reductase) and PfK13 propeller (Plasmodium falciparum Kelch13 propeller) genes. The amplification products were processed by electrophoresis and analyzed against blood, saliva and urine samples. A multivariate statistical analysis in R programming environment was performed aiming to assess the performance of blood, saliva and urine samples in detecting molecular markers of P. falciparum resistance. Results: Agarose gel electrophoresis of the amplification products of each gene detected the Pfcrt genes at 80.85% (76/94), Pfdhfr at 95.74% (90/94) and PfK13 Propeller at 98.93% (93/94) in blood. In saliva, gene detection levels were 50% (47/94), 69.14% (65/94) and 4.26% (4/94) respectively for the K13 propeller, Pfdhfr and Pfcrt genes. Unlike the Pfcrt gene, which was not detected, 45.74% (43/94) and 38.30% (36/94) of PfK13 Propeller and pfdhfr genes respectively were detected in urine. Taking blood as the reference biological sample, statistical analysis showed that unlike urine, saliva exhibited a detection performance for molecular markers of antimalarial drug resistance (pfcrt, pfdhfr, pfK13 propeller) close to that of blood (p pfdhfr, pfcrt and pfK13 using ROC (receiver operational characteristic) analysis. The data revealed a high sensitivity of saliva compared with urine in the detection of the pfdhfr, pfcrt and pfK13 propeller genes. Conclusion: The levels of detection of molecular markers of antimalarial drug resistance studied in saliva are close to those in blood. Saliva is a high-performance biological product that could potentially be used as an alternative non-invasive sample for the study of molecular markers of Plasmodium falciparum resistance to antimalarial drugs. VL - 9 IS - 3 ER -
Biosciences Training and Research Unit (UFR), Felix Houphouët-Boigny University, Abidjan, Côte d’Ivoire; Department of Parasitology-Mycology, Pasteur Institute of Côte d’Ivoire, Abidjan, Côte d’Ivoire
Training and Research Unit (UFR) of Biological Sciences, Peleforo Gon Coulibaly University, Korhogo, Côte d’Ivoire
Biosciences Training and Research Unit (UFR), Felix Houphouët-Boigny University, Abidjan, Côte d’Ivoire; Department of Parasitology-Mycology, Pasteur Institute of Côte d’Ivoire, Abidjan, Côte d’Ivoire
Department of Parasitology-Mycology, Pasteur Institute of Côte d’Ivoire, Abidjan, Côte d’Ivoire
Biosciences Training and Research Unit (UFR), Felix Houphouët-Boigny University, Abidjan, Côte d’Ivoire
Training and Research Unit (UFR) of Biological Sciences, Peleforo Gon Coulibaly University, Korhogo, Côte d’Ivoire
Biosciences Training and Research Unit (UFR), Felix Houphouët-Boigny University, Abidjan, Côte d’Ivoire; Department of Parasitology-Mycology, Pasteur Institute of Côte d’Ivoire, Abidjan, Côte d’Ivoire
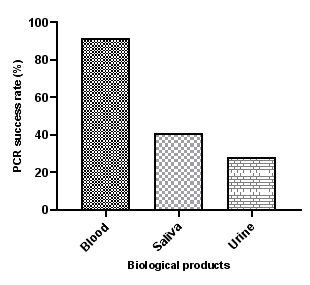
Figure 1. PCR success rate as a function of the biological product.
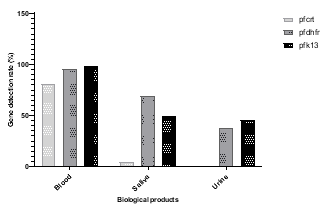
Figure 2. Detection rate of gene fragments by biological product.
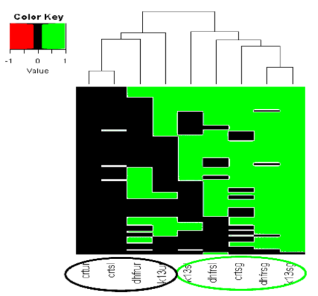
Figure 3. Graphical monitoring of the expression of the pfK13 propeller, pfdhfr and pfcrt genes in blood, saliva and urine extracts for the molecular diagnosis of malaria.
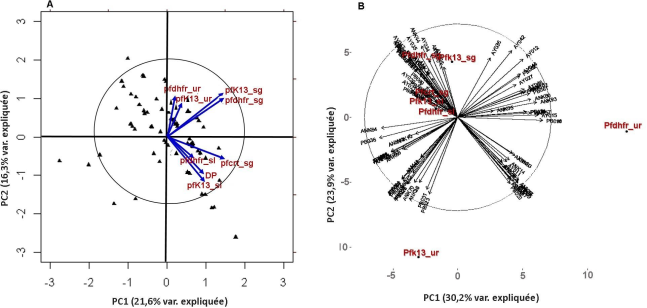
Figure 4. Comparative analysis of the relationship between the pfk13 propeller, pfdhfr, and pfcrt genes detected in blood, saliva and urine samples.
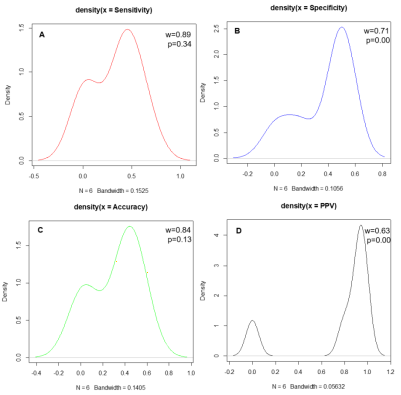
Figure 5. Shapiro normality test for assessing the distribution of urine and saliva samples statistical performance parameters.
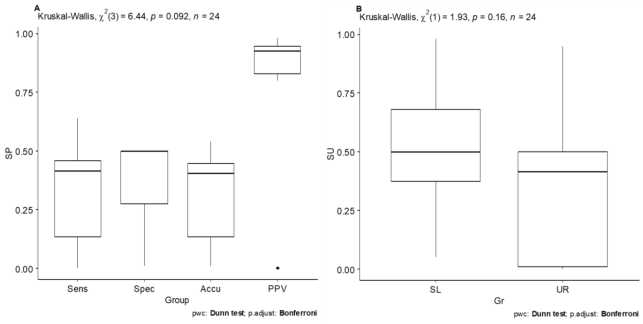
Figure 6. Kruskal-Wallis test evaluating statistical parameters variability (A) by comparing saliva and urine performances (B) in malaria molecular diagnosis procedure in alternative to blood sample.

